

A patient with worsening heart-failure symptoms messages her clinic portal late on a Sunday. No clinician reads it until Monday morning; meanwhile her condition deteriorates.
Now picture a different version, where within seconds, a software system reads her message, pulls her record, compares the pattern against her last three visits, drafts a triage note, books an urgent appointment, and routes the case to the on-call nurse for review before anyone pours a coffee.
That second version describes agentic AI in healthcare.
Agentic AI in healthcare means software that plans and carries out multi-step tasks toward a goal, then pauses for human sign-off, instead of waiting for a prompt at each step.
It differs from a chatbot, which answers and waits, and from rule-based automation (like healthcare RPA), which breaks when a workflow changes.
Today, agentic AI systems do their best work on administrative load: ambient note-taking, prior authorization, billing codes, scheduling, and follow-up.
Clinical decision support and triage exist too, though they keep a clinician in the loop.
Adoption has climbed fast on paper; in practice, most healthcare organizations run pilots and few run agents in production.
Regulators have started to move, with the FDA, EU, UK, and several US states drawing early lines around autonomy and human oversight.
The hardest unresolved questions concern liability and patient safety when an agent gets something wrong.
For any healthcare provider weighing this, a useful test asks four things: what the agent’s scope covers, where it escalates, how reliable the underlying data is, and what happens when it errs.

What agentic AI in healthcare means
The term causes confusion, even in the literature. A 2026 scoping review in npj Digital Medicine found that published work often fails to separate “AI agents” from “agentic AI.”
Agentic AI falls along an autonomy spectrum.
So start with function. A generative AI tool writes a discharge summary when you ask. An agentic AI system writes the summary, checks it against the chart, spots a missing lab, orders the follow-up for a clinician to approve, and updates the record.
The difference lies in initiative and in chaining several steps without a fresh instruction for each one.
Three properties recur across credible descriptions:
- The system pursues a goal
- It plans and acts across tools, and
- It adapts when conditions change.
None of that removes the clinician, but it changes what reaches them, and when.
| Capability | Rule-based automation | Generative AI | Agentic AI |
| Responds to | Fixed triggers | A prompt | A goal |
| Takes action | Within strict rules | Produces text | Plans and runs steps |
| Handles change | Breaks | Needs re-prompting | Adapts within limits |
Why this is surfacing now
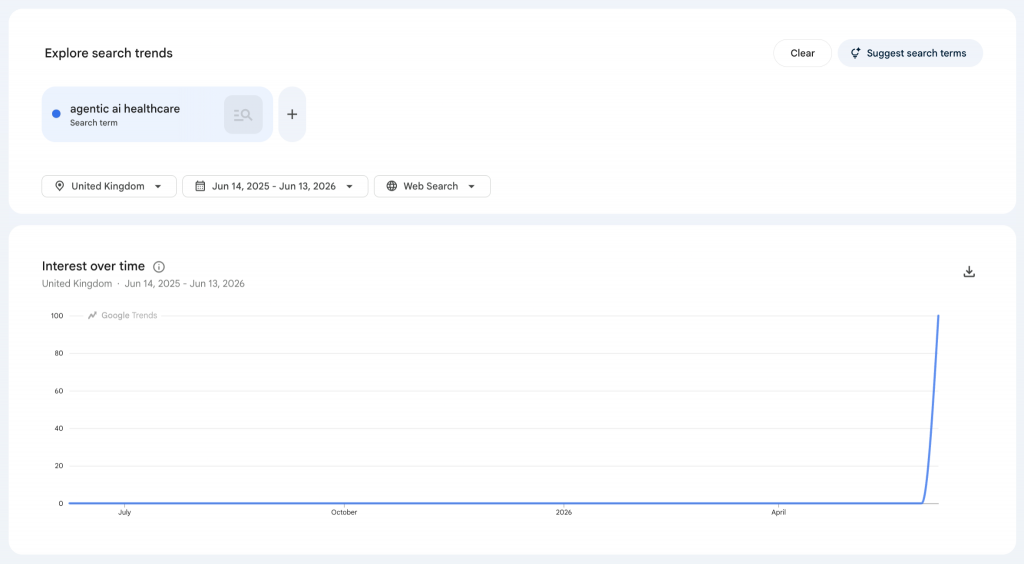
Search interest in agentic AI healthcare has climbed because the technology has moved out of the lab and because the pressure to use it has grown.
In the UK specifically, interest has spiked in recent weeks, suggesting a change in how the local healthcare industry is approaching care delivery.
Hospitals and other healthcare organizations carry heavy documentation and administrative burden, and staffing hasn’t kept pace.
Healthcare leaders across the wider sector now weigh agentic systems as a way to cut costs and protect patient outcomes.
Surveys give us a sense of the appetite. In Deloitte’s 2026 US health-care survey, 61% of executives said they were already building agentic AI or had secured budget for it.
McKinsey’s late-2025 work found 19% of healthcare organizations had reached agentic AI implementation, with 51% running proofs of concept.
Separate research from Microsoft and the Health Management Academy, published in the New England Journal of Medicine, found only 3% of provider organizations had agents in live workflows (43% were piloting or testing agentic AI).
The interest runs ahead of the practice, and most healthcare systems now focus on implementing agentic AI safely across clinical workflows.
Agentic AI use cases and case studies in healthcare systems
The clearest agentic AI use cases today reduce paperwork rather than make diagnoses, though they reach across patient care and the wider healthcare workflow.
At AtlantiCare in New Jersey, an early Oracle Health Clinical AI Agent deployment reached about 80% adoption among its first providers, who saved roughly 66 minutes a day on notes.
Administrative agents run prior authorization, eligibility checks, and medical coding end to end, flagging the exceptions a person needs to see.
On the clinical side, healthcare AI agents support triage and clinical decision support by reading patient data, ranking risk, and surfacing evidence for treatment plans, while leaving the call to a clinician.
Patient-facing agents handle scheduling, reminders, and patient information requests, and some draft personalized treatment plans for a clinician to approve.
Specialized agents watch one task, such as sepsis alerts or patient monitoring.
A broader agentic system chains several of these into one agentic workflow, and bigger agentic systems coordinate the whole care team across busy healthcare environments.
Drug discovery and research use agents too, though that work runs apart from direct patient care.
Across these healthcare AI solutions, the general pattern is of an agent moving the task forward, then handing off before the decision that carries clinical risk.
| Domain | What the agent does | Stage today |
| Documentation | Drafts visit notes and discharge summaries for review | In production |
| Administration | Runs prior authorization, medical coding, claims, and routine administrative tasks | Scaling |
| Clinical decision support | Reads the chart, ranks risk, cites evidence for clinical decision-making | Piloted, clinician-led |
| Care coordination | Syncs the care team, updates electronic health records and patient records | Early |
| Patient engagement | Manages scheduling, reminders, and patient monitoring between visits | Growing |
How big is the market for AI healthcare agents?
Estimates vary widely, because firms scope “agentic AI in healthcare” differently.
Grand View Research valued the 2024 market near $538.5 million; other firms put 2025 closer to $1.5 billion.
Most forecasts agree on direction, projecting growth past $33 billion by 2035, with buyers comparing point tools and full agentic AI solutions.
Most published results so far report time saved and cost reduced. Less firm evidence exists yet on patient outcome and care delivery across the whole healthcare system.
These figures sell reports, so read them as momentum signals, not exact counts.
The risk and governance questions of implementing agentic AI
Three classes of risk recur when exploring an agentic system for a healthcare organization.
First, errors. An AI agent that drafts a wrong note, misreads a chart, or proposes a flawed billing code can push a mistake downstream. In multi-agent setups, an error in one administrative task can spread to others.
Second, accountability. When an agent’s action contributes to harm or loss, the law hasn’t settled who answers for it: the clinician, hospital, or vendor.
A 2026 arXiv analysis argues that the “agentic” label often over-promises autonomy while leaving responsibility unclear when something goes wrong.
Third, data and privacy. These systems reach across patient data and electronic records, which widens the surface for leaks and bias, and raises the bar for patient safety.
Regulators have begun to respond. The FDA now uses agentic AI internally and defines it around planning, reasoning, and multi-step action with built-in human oversight; its own staff assistant, Elsa, reached more than 70% use within months.
The EU AI Act, through Article 14, requires high-risk AI to be designed so people can oversee, interpret, and halt it.
The UK has gone a different way, with no single AI Act: its medicines regulator, the MHRA, treats clinical AI as a medical device and runs the AI Airlock sandbox, which secured £3.6 million in 2026 (£1.2 million per year through 2029).
In the US, Illinois passed the Wellness and Oversight for Psychological Resources Act in 2025, which bars AI from making independent therapeutic decisions in mental health care without a licensed professional’s review.
All four share one requirement—human oversight—which decides where autonomy stops.
What to ask before adopting an agentic AI solution in healthcare
Before a healthcare provider buys or builds an agentic AI solution, four questions help cut through the noise.
- What scope does the agent own, and what does it never touch?
- Where does it escalate, and to whom?
- How complete and reliable is the data it depends on, since a capable agent on poor data produces confident errors (hallucinations)?
- And what happens when it gets something wrong: who catches it, how fast, and who carries the liability?
Healthcare leaders should start narrow, on one workflow or administrative task with clear value, then measure against a baseline before they widen scope.
The right AI agent framework can speed up implementation, reduce administrative costs, and minimize risks.
Match the autonomy to the clinical risk, have a defined AI governance framework in place (like ISO 42001), and keep healthcare professionals involved on every step that touches diagnoses or treatment plans.
Where agentic AI goes next for the healthcare industry
The near-term direction points toward coordinated multi-agent systems and tighter rules rather than full autonomy.
For now, agentic AI in healthcare does its surest work at the edges of care delivery, clearing administrative load so clinicians spend more time with patients.
Across the sector, wider healthcare transformation will depend on evidence, governance, and clinical trust keeping pace, and on agentic systems proving they improve healthcare delivery and patient safety.
To map your current clinical or administrative workflows before implementing agentic AI solutions, book an audit today.